The Cure Was the Disease
In 1847 Vienna, the doctors’ maternity ward killed far more mothers than the midwives’. Ignaz Semmelweis found the cause, and it was the one thing the profession could not afford to believe: their own hands.
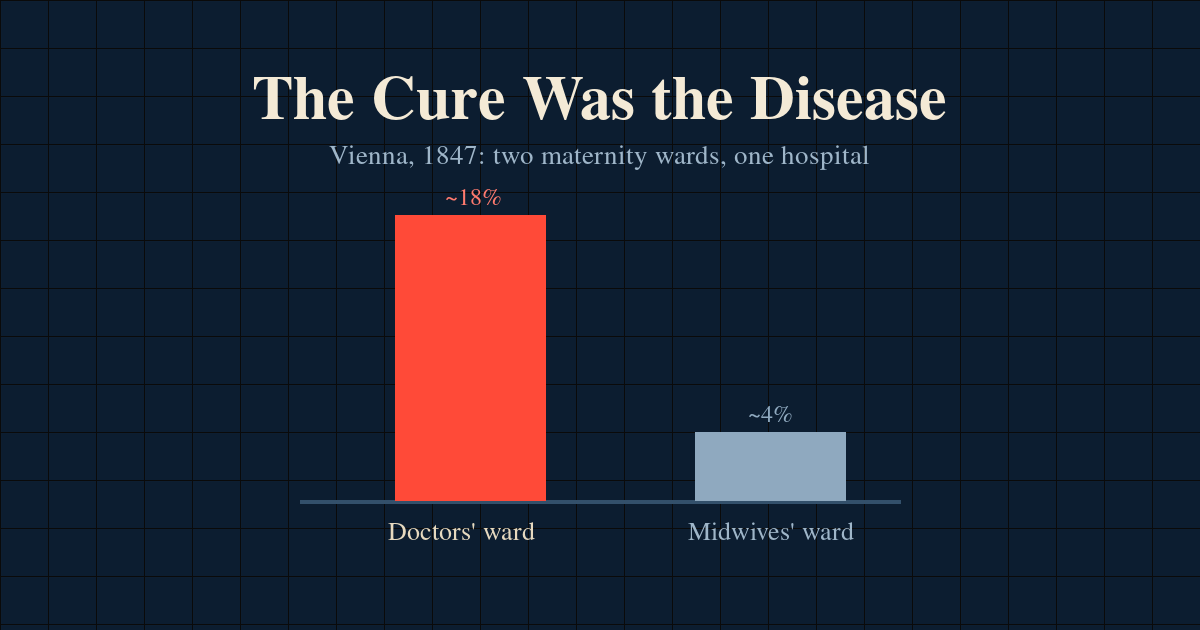
In the Vienna General Hospital of the 1840s, where a woman gave birth was decided by the calendar. The maternity service ran two clinics, side by side in the same building, and they admitted in turn: one clinic took the women who arrived on one day, the other took the next day’s. Which ward received you came down to nothing but the date your labour began. The first clinic was run by doctors and medical students. The second by midwives. In the obvious respects, the two seemed comparable. The same building, the same air, the same city, the same women, sorted between the wards by the calendar alone.
And yet the first clinic killed mothers at two to three times the rate of the second. In its worst months it lost more than one woman in six.
The women knew. They learned to dread the doctors’ days and prayed to be admitted on the midwives’. Some, told they were bound for the first clinic, wept and pleaded. A few gave birth deliberately in the street and then arrived claiming the baby had come early, because a birth on the cobbles was safer than a clean bed in the first clinic. They were not being superstitious. They were reading the pattern more honestly than the physicians who explained it away.
The killer was puerperal fever, childbed fever: a fast, sweating sepsis that could take a healthy woman within days of an uncomplicated delivery.
A puzzle nobody wanted solved
Ignaz Semmelweis, a young Hungarian doctor, took a post in the first clinic in 1846. The gap between the two wards was not a secret. It was an embarrassment, and embarrassments attract explanations.
The reigning theory was miasma: a vague atmospheric influence, bad air settling over a ward. But the same air sat over both clinics. Overcrowding was blamed, except the second clinic was the more crowded of the two, precisely because women fought to get into it. The rough handling of male students was blamed, and the women’s wounded modesty, and even a priest: he passed through the first clinic ringing a bell to deliver last rites, and it was said the sound so terrified the labouring women that it brought on the fever. Semmelweis sent the priest by another route and silenced the bell. Nothing changed.
Each explanation had one quiet thing in common. Every one of them located the cause somewhere safe. In the air, in the building, in the patients, in the priest. None of them looked at the doctors.
The death that gave it away
The answer came from a death that had nothing to do with childbirth.
In 1847 Semmelweis’s friend and colleague Jakob Kolletschka was cut on the finger by a student’s scalpel during a post-mortem. He sickened and died, and the findings at his own autopsy looked, to Semmelweis, exactly like the disease killing the mothers upstairs. The same fever, the same internal picture.
Kolletschka had never been pregnant. He had simply been cut with a blade fresh from a corpse.
That was the hinge. The doctors and students of the first clinic spent their mornings dissecting the dead, then walked upstairs and examined labouring women, often without washing in between. They were carrying something Semmelweis called “cadaverous particles” from the autopsy room into the birth canal. The midwives of the second clinic did no dissections. That single difference, invisible because it was so ordinary, was the difference between the two wards.
Stated plainly, the cause of the deaths was the people investigating them. The doctors were not the disease itself; they were its vector, carrying it from the dead to the living on unwashed hands. The cure and the contagion arrived in the same pair of hands.
The assumption no one would touch
It is worth being precise about where the error lived, because it was not where you would expect.
The question the profession asked was the right one: what causes childbed fever? The data they had was real. The logic they applied to it was not obviously broken. The fatal move was one layer underneath, in a premise so deep that nobody experienced it as a premise at all:
A physician’s hands are clean.
Not clean as in recently washed. Clean as in incapable of being the source. The doctor was a healer, a gentleman, an educated man. The American obstetrician Charles Meigs later gave that attitude its perfect sentence: “But a gentleman’s hands are clean.” That was the load-bearing assumption. Every accepted explanation for the deaths was built on top of it, and every one of them had to be, because the alternative was unthinkable.
Semmelweis relaxed the one assumption his colleagues could not. He allowed himself to ask whether the cause might be the doctors themselves. The instant he did, the noise resolved into a single signal. The two wards, the crowded-but-safer midwives, the priest with his bell, the dead friend on the dissecting table: all of it became one explanation.
In May 1847 he ordered the doctors of the first clinic to wash their hands in a solution of chlorinated lime before examining patients. The death rate collapsed. A ward that had been losing women at something near eighteen per cent in its worst stretch fell to around one per cent. The alternate-day rota had, by accident, set up something close to a controlled comparison, and the handwashing turned it into a test. Change one thing, wash the hands, and the dying fell away.
He had the question, the data, the mechanism, and the result. He should have won.
Why being right was not enough
He did not win. The profession, for the most part, did not accept him, and it is tempting to put that down to vanity alone. The truth is less tidy, and more useful.
Semmelweis was right, but not perfectly right. He had the practice, wash your hands, without the theory. Germ theory did not yet exist, so he could not say what the morbid matter was, or why it killed, only that corpses were somehow involved. He was also slow to publish, left his evidence poorly set out for years, and when he finally laid it down he wrapped it in a difficult, combative style, then took to writing open letters branding his critics as murderers. Some of the resistance he met was earned. A careful contemporary had real grounds to call the case suggestive but unproven.
So this is not a fable of one genius against a room of fools. The objections were partly legitimate. But beneath every legitimate objection sat one possibility the objectors could not bring themselves to entertain, and it was the true one: that the doctors themselves were the mechanism.
The premise that the physician could not be the carrier was not a hypothesis held lightly, to be revised when the data came in. It was structural. It propped up the doctor’s standing, his training, his sense of himself as the cure and not the contagion. To relax it was not merely to lose an argument. It was to accept that the healer had also been the mechanism of harm.
This is the pattern worth carrying out of the story. The assumption that killed those mothers was not exotic, and it was not stupid. It was protected. It was load-bearing for the self-image of the very people who would have had to give it up. An assumption that flatters you is almost impossible to see as an assumption at all, because doubting it means doubting yourself.
The deadliest assumptions flatter the people holding them.
There is even a name for the response Semmelweis met, borrowed from his ordeal: the Semmelweis reflex, the reflexive rejection of evidence that contradicts an established belief or a comfortable identity. Some assumptions are bracketed, seen clearly and used anyway; this kind is the opposite, invisible precisely because status protects it. The premise you would be most ashamed to hold is the one you are least able to notice you are holding.
The cost
Vindication did not come in his lifetime. His mind gave way under the strain and the grief, and in 1865 he was committed to an asylum. He died there within weeks, at the age of forty-seven, of an infected wound that turned septic, the same kind of infection he had spent his life trying to stop.
The mechanism arrived only after his death, when Pasteur, Lister, and Koch named what he had lacked: germs. Semmelweis had been wrong about the precise agent. He thought in terms of cadaverous particles, not living microbes. But he had been right about the only thing that mattered to the women in his care. Wash your hands.
What to take from it
You are not a Vienna obstetrician. But you hold assumptions that are load-bearing for who you believe yourself to be. Those are the ones you defend hardest and inspect least, because the cost of being wrong is not merely intellectual. It is personal.
So here is the move the story hands you. When the honest answer to a problem would require you to be the cause, notice the flinch. The reluctance is not evidence that the answer is wrong. It is often evidence that you have found the load-bearing assumption.
What if it is us?
Sources
- Ignaz Semmelweis, Die Aetiologie, der Begriff und die Prophylaxis des Kindbettfiebers (The Etiology, Concept and Prophylaxis of Childbed Fever), 1861.
- Sherwin B. Nuland, The Doctors’ Plague: Germs, Childbed Fever, and the Strange Story of Ignác Semmelweis (2003).
- K. Codell Carter and Barbara R. Carter, Childbed Fever: A Scientific Biography of Ignaz Semmelweis.
- On the “Semmelweis reflex”: the term for reflexive rejection of evidence that contradicts established norms, named for his reception.